
The view of a builder of future geniuses in the reproductive field.
By Lucy Coleman and Kevin Coward.

Kevin Coward is a colleague and friend who I admire a lot. I met Kevin about 10 years ago in Oxford. We were both seating at the same desk writing and reading papers non-stop, talking about interesting projects and our wishes for the future. He was offered the role as Director of the MSc. Course in Embryology at Oxford University in England – UK, and I ended up specializing in reproductive medicine and embryology.
His embryology course is one of the best and most wanted around the world, because of the quality of professors and teaching techniques they use.
Celine Jones (with us in the photo) has been an amazing collaborator as well. They both were awarded with the Ox Talent award (Teaching and learning enhanced by New Technology) for innovative use of technology recently in 2013.
Dr. Kevin Coward has a PhD in Reproductive Physiology and Endocrinology from the University of Stirling in Scotland. He has gained lots of experience in the reproductive field working alongside several well-known researchers, and is now working in several projects with sperm and eggs.
He was kind enough to answer some questions to provide an insight on the goals and achievements from someone who has spent his entire life dedicated to research and innovative techniques that might one day revolutionise the world of reproductive medicine.
What is your vision of current research regulations in the UK? Are they necessary? What would happen if there were no regulations?
Fertility treatment and research using reproductive material is regulated in the UK by the Human Fertilisation and Embryology Authority. Further regulation is imposed by the National Research Ethics Service, and by the Human Tissue Act. Collectively, this three-tier approach ensures that scientists and clinicians can only use human cells and tissues in research projects for specific goals using specific techniques. This also ensures that material can only be used when patients have given informed written consent, and have been given detailed patient information sheets describing in simple terms what is happening to their cells/tissue, how, why, and who is involved. Without such regulation, there would be no requirement for peer-review (as would normally happen by both HFEA and NRES Committees which include scientists, clinicians, and members of the general public) and therefore, patient samples (including DNA) could be used indiscriminately for a whole range of projects that had not been sanctioned or scrutinised. This could easily lead to the exchange of patient material between research groups, or between countries, possibly in response to financial arrangements, and without the donating patient knowing.
Do you think a worldwide regulation for research would be beneficial?
Yes. This would promote significant reproducibility and consistency in the way in which scientists approached their clinical work and readily encourage collaborative ventures. Ultimately, such a regulated and consistent approach would directly lead to improved patient care and treatment outcome.
There are many issues and different points of view regarding egg and embryo research. Is that a controversial subject?
Very controversial and highly variable when one considers the global position. Some countries adopt highly regulated approaches while others do not. Regulation prevents the indiscriminate use of human material in research, ensures that the research being carried out is warranted and worthwhile, and promotes confidence and reproducibility in results, while protecting patient interests and anonymity.
Are there any recommendations to people in the reproductive field looking to do research?
Ensure that one approaches research with an informed and robust attitude. Ensure research projects are warranted and worthwhile. Ensure that systematic literature reviews, along with experimental design and tests of the statistical power required for proof-of-principle, are carried out before the research programme is commenced. Encourage peer-review of all research projects. Ensure that material is acquired, stored, and utilised in a regulated manner and that appropriate levels of research governance are imposed – such as secure data management and protection of all personalised patient data. Encourage blinded research and the use of appropriate controls. Promote intense peer-review of all publications arising from research. Encourage regular review of all procedures and policies.
Where are we going to with reproductive research?
Research in our field aims to promote our understanding of human infertility both in terms of the mechanisms underlying such problems and the development or modification of treatment options to circumvent such issues. We do this by developing new hypotheses, technologies and equipment, or by modifying existing techniques or equipment from other fields in line with scientific advancement. Collectively, research at the clinical and basic science level, aims to promote better diagnostic and treatment options for patients, to improve treatment outcome, and to provide patients with the best levels of care.
Is there any messages to the general public regarding what we are doing with reproductive research?
In general, all research effort in our field, aims to promote improved levels of diagnosis and treatment and to improved treatment outcome. Essentially, everything we do is driven by the need to provide patients with the best level of care at all times.
Venezuela has no regulations or legislation in fertility practices. Should we propose to be regulated or is it better not to have control?
Yes. I think it is critical that Venezuela adopts appropriate research and clinical legislation based upon established systems such as that of the Human Fertilisation and Embryology Authority (HFEA) in the UK. From the patient’s perspective, regulation provides the security and understanding that the procedures and techniques being used have been fully optimised and risk-assessed and that all medical personnel are carrying out such procedures in a standardised manner. This will prevent the risk of malpractice and instil confidence in the industry. This will also encourage patients to contribute to research projects and attract attention from potential collaborators overseas. This would promote the clinical research profile of Venezuela.
 Do you consider yourself an innovative person?
Do you consider yourself an innovative person?
Absolutely. I rigorously adopt innovation and resourcefulness in both my research and teaching practice as this is the only way to teach and inform others of a subject area that exhibits such dynamic changes as ours. From a research point of view, innovation is a key requirement in order to maintain originality and motivate fellow researchers.
Having done this job as a head of an MSc course in embryology, might had given you lots of experiences to talk about.
Can you discuss some of the most relevant?
I have enjoyed my job immensely over the last five years and I learn something new from every different class I teach. In five years, we have had representatives from over 28 different countries. The approach to human infertility treatment varies significantly across the world and many of our students join our course in order to appreciate the UK’s approach to the treatment, diagnostics, along with regulatory, legal, and ethical aspects of treatment and to translate this information back to their host nations. In doing this, our students are adopting an admirable strategy and encouraging a consistent approach. We now have graduates all over the world, who, in effect, act as ambassadors for the field in the promotion of good practice. It has been an honour to be involved and I will never tire of witnessing the motivation, inspiration and resilience of our students.
Many people consider fertility specialists to go against nature. What do you think about this statement?
It is of course entirely understandable that our field is questioned on religious, ethical and moral grounds. However, the facts are now very clear – over 1 in 7 couples globally are now classified as being infertile. That is, they are unable to achieve the one thing that many deem to be the most natural event in one’s life – that of producing progeny. The effect of infertility is highly emotional and traumatic for those concerned. In many cases, the desire to have a child out-weighs all over life goals. We now have the ability to rescue fertility in many cases in a safe, regulated, and consistent manner. I think it is therefore down to the individual as to whether they see our field as being controversial or going against nature. At the end of the day, it is the choice of the infertile couple that is important – they can either choose to go ahead or not. If my research can help even a small number of couples achieve the one thing they desire so much but cannot produce naturally, then my time and effort has been well spent.
 “CUANDO EL MUNDO SE DIBUJA DETRÁS DE UNA SONRISA”.
“CUANDO EL MUNDO SE DIBUJA DETRÁS DE UNA SONRISA”. Los niños con síndrome de Down, tienen una característica común, son muy tiernos, muy serviciales, abnegados y profundamente inteligentes, NUNCA DEBEMOS DISCRIMINARLOS, hay que hacerles ver lo importantes que son, y sobre todo brindarles oportunidades de superación y trabajo. Son excelentes atletas, los más responsables en el trabajo y en todo lo que hacen, porque su única misión en el mundo es llenar de alegría a aquellos Ángeles que aun sabiendo de su trastorno genético, le dieron la oportunidad de llenar su hogar y su vida con muchas sonrisas.
Los niños con síndrome de Down, tienen una característica común, son muy tiernos, muy serviciales, abnegados y profundamente inteligentes, NUNCA DEBEMOS DISCRIMINARLOS, hay que hacerles ver lo importantes que son, y sobre todo brindarles oportunidades de superación y trabajo. Son excelentes atletas, los más responsables en el trabajo y en todo lo que hacen, porque su única misión en el mundo es llenar de alegría a aquellos Ángeles que aun sabiendo de su trastorno genético, le dieron la oportunidad de llenar su hogar y su vida con muchas sonrisas. El embarazo es una condición fisiológica que produce una serie de cambios en la mujer, no solo es el hecho de ver cómo crece poco a poco tu abdomen y te sientes un poco más gordita, de pronto te sientes hinchada, muy sentimental, te va costando poco a poco ir al baño, y muchas otras cosas.
El embarazo es una condición fisiológica que produce una serie de cambios en la mujer, no solo es el hecho de ver cómo crece poco a poco tu abdomen y te sientes un poco más gordita, de pronto te sientes hinchada, muy sentimental, te va costando poco a poco ir al baño, y muchas otras cosas. Nos encontramos en una lucha constante y que en las últimas décadas ha mostrado avances prometedores contra la enfermedad del Cáncer. Son millones de personas anualmente que siguen muriendo por esta causa, y muchos científicos se han dedicado a resolver los antes llamados enigmas de esta enfermedad; hoy ya resueltos los enigmas las investigaciones van dedicadas a encontrar su cura.
Nos encontramos en una lucha constante y que en las últimas décadas ha mostrado avances prometedores contra la enfermedad del Cáncer. Son millones de personas anualmente que siguen muriendo por esta causa, y muchos científicos se han dedicado a resolver los antes llamados enigmas de esta enfermedad; hoy ya resueltos los enigmas las investigaciones van dedicadas a encontrar su cura. Carolina L.: Yo soy abogada y solía trabajar muchísimo para ayudar a mis colegas y resolver todos los casos posibles en materia penal. Siempre visitaba las cárceles para ofrecer consultas a los presos que muchas veces eran inocentes o muchos de ellos tienen problemas familiares que los llevaron a cometer crímenes menores y que luego llegaban a esas cárceles con criminales verdaderos y se convertían en criminales de alto riesgo ellos mismos. Era una situación de locura que siempre me llamó la atención. La adrenalina me motivaba a seguir trabajando y trabajando. Me gradué a los 23 años y cuando me di cuenta que era hora de comenzar una familia ya tenía 35 años. Fueron relaciones que ninguna servía y me fui decepcionando de cada uno de los candidatos que entraban a mi vida para tener una relación. Y un buen día decidí congelar mis óvulos. Leí unos artículos muy interesantes acerca de conservar las células germinales por medio de la congelación y fue lo que decidí hacer. Pensaba que los usaría en cuanto encontrara el candidato. Pero lo que encontraron en mi fue un inmenso tumor de mamas. Mi abuela había tenido lo mismo pero no pensé que me podría suceder. Luego leí mucho mas y me entere que esa enfermedad corre en la familia y que mi genética provenía de la misma genética de mi abuela y materna, por lo que yo tenía mucho chance de sufrir la enfermedad. Pero nadie me había dicho esto antes. No es una información que mi ginecólogo me daba. Yo solo lo leí en un artículo y así fue que cuando me dieron la noticia pues ya sabía que hacer. Tuve que realizarme varias quimioterapias y mis médicos me dijeron que un efecto secundario sería el quedar estéril inmediatamente. Entonces entendí todo. Entendí que el congelar mis óvulos fue una señal de Dios.
Carolina L.: Yo soy abogada y solía trabajar muchísimo para ayudar a mis colegas y resolver todos los casos posibles en materia penal. Siempre visitaba las cárceles para ofrecer consultas a los presos que muchas veces eran inocentes o muchos de ellos tienen problemas familiares que los llevaron a cometer crímenes menores y que luego llegaban a esas cárceles con criminales verdaderos y se convertían en criminales de alto riesgo ellos mismos. Era una situación de locura que siempre me llamó la atención. La adrenalina me motivaba a seguir trabajando y trabajando. Me gradué a los 23 años y cuando me di cuenta que era hora de comenzar una familia ya tenía 35 años. Fueron relaciones que ninguna servía y me fui decepcionando de cada uno de los candidatos que entraban a mi vida para tener una relación. Y un buen día decidí congelar mis óvulos. Leí unos artículos muy interesantes acerca de conservar las células germinales por medio de la congelación y fue lo que decidí hacer. Pensaba que los usaría en cuanto encontrara el candidato. Pero lo que encontraron en mi fue un inmenso tumor de mamas. Mi abuela había tenido lo mismo pero no pensé que me podría suceder. Luego leí mucho mas y me entere que esa enfermedad corre en la familia y que mi genética provenía de la misma genética de mi abuela y materna, por lo que yo tenía mucho chance de sufrir la enfermedad. Pero nadie me había dicho esto antes. No es una información que mi ginecólogo me daba. Yo solo lo leí en un artículo y así fue que cuando me dieron la noticia pues ya sabía que hacer. Tuve que realizarme varias quimioterapias y mis médicos me dijeron que un efecto secundario sería el quedar estéril inmediatamente. Entonces entendí todo. Entendí que el congelar mis óvulos fue una señal de Dios. Sandra Y. : Tengo 39 años y quisiera compartir mi historia con ustedes. Me diagnosticaron cáncer de cuello uterino y comenzar con las quimioterapias de inmediato. No era aconsejable usar hormonas porque los tumores se alimentan de ellas. Comencé a investigar y supe de la congelación de óvulos y embriones. Acudí a una clínica donde me aconsejaron que podía congelar mis embriones pero requería de una preparación hormonal que podía empeorar mi cáncer y que era mi decisión realizarlo o no. Pues decidí seguir adelante y someterme a la estimulación con hormonas y logramos congelar 12 embriones con mi esposo. Al día siguiente comencé con las quimioterapias y el médico me dijo que el cáncer había empeorado. Sin embargo yo todos los días rezaba a Dios por mi mejoría y porque mis hijos estaban allí esperando por mi. Así que me armé de valor para lograrlo y comencé a mejorar. Los médicos estaban impresionados conmigo. Todos los meses hablaba con las doctoras de Fertiaguerrevere para contarles que estaba mejorando y que por favor cuidaran a mis bebes. Ellas me decían que allí estaban ellos esperando por mi. Incluso una vez fui a visitarlos y quise hablarles de mi mejoría. Luego de casi dos años mi médico me dijo que ya estaba lista para intentarlo y lo hice, me puse mis embriones. Quedé embarazada y tengo dos bellos bebes. Logree ser mamá luego de vencer al cáncer y quiero que ellos sepan que soy una luchadora y que tienen que aprender eso de mi. Gracias a todos mis médicos y a Fertiaguerrevere por todos los consejos y horas dedicadas conmigo. Las quiero mucho doctoras.
Sandra Y. : Tengo 39 años y quisiera compartir mi historia con ustedes. Me diagnosticaron cáncer de cuello uterino y comenzar con las quimioterapias de inmediato. No era aconsejable usar hormonas porque los tumores se alimentan de ellas. Comencé a investigar y supe de la congelación de óvulos y embriones. Acudí a una clínica donde me aconsejaron que podía congelar mis embriones pero requería de una preparación hormonal que podía empeorar mi cáncer y que era mi decisión realizarlo o no. Pues decidí seguir adelante y someterme a la estimulación con hormonas y logramos congelar 12 embriones con mi esposo. Al día siguiente comencé con las quimioterapias y el médico me dijo que el cáncer había empeorado. Sin embargo yo todos los días rezaba a Dios por mi mejoría y porque mis hijos estaban allí esperando por mi. Así que me armé de valor para lograrlo y comencé a mejorar. Los médicos estaban impresionados conmigo. Todos los meses hablaba con las doctoras de Fertiaguerrevere para contarles que estaba mejorando y que por favor cuidaran a mis bebes. Ellas me decían que allí estaban ellos esperando por mi. Incluso una vez fui a visitarlos y quise hablarles de mi mejoría. Luego de casi dos años mi médico me dijo que ya estaba lista para intentarlo y lo hice, me puse mis embriones. Quedé embarazada y tengo dos bellos bebes. Logree ser mamá luego de vencer al cáncer y quiero que ellos sepan que soy una luchadora y que tienen que aprender eso de mi. Gracias a todos mis médicos y a Fertiaguerrevere por todos los consejos y horas dedicadas conmigo. Las quiero mucho doctoras. En Fertiaguerrevere tenemos muchos casos e historias hermosas ó algunas tristes pero llenas de coraje. Felicitamos a todos los pacientes que deciden luchar y respaldarse con sus células germinales. Las situaciones de la vida pueden cambiar dramáticamente de un día para otro. Lo importante es luchar y no darse por vencido. Así como nuestros pacientes han logrado sus sueños ustedes también pueden. Todo es cuestión de actitud.
En Fertiaguerrevere tenemos muchos casos e historias hermosas ó algunas tristes pero llenas de coraje. Felicitamos a todos los pacientes que deciden luchar y respaldarse con sus células germinales. Las situaciones de la vida pueden cambiar dramáticamente de un día para otro. Lo importante es luchar y no darse por vencido. Así como nuestros pacientes han logrado sus sueños ustedes también pueden. Todo es cuestión de actitud.
 1. What do you think about fertility tourism and the implications of this? Does it have something to do with fertility regulations, or do you think that there are regulations affecting the vision of reproductive specialists?
1. What do you think about fertility tourism and the implications of this? Does it have something to do with fertility regulations, or do you think that there are regulations affecting the vision of reproductive specialists?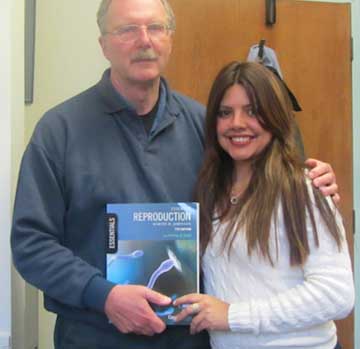 On April 2013, I decided to pay a visit to Prof. Martin Johnson at Cambridge University. He has had a broad trajectory in the fertility field, and is one of the original developers of the guidelines for the Human Fertilization and Embryology Authority (HFEA).
On April 2013, I decided to pay a visit to Prof. Martin Johnson at Cambridge University. He has had a broad trajectory in the fertility field, and is one of the original developers of the guidelines for the Human Fertilization and Embryology Authority (HFEA). En muchas oportunidades cuando me encuentro dentro de mi laboratorio de fertilidad siento que no podría estar en otro sitio donde esté mas feliz. Es una sensación única de plena paz. En ese lugar puedo meditar, siento vida y encuentro el sentido para muchas de mis interrogantes. Cuando miro mi vida hacia atrás pienso que no existe nada mas que me hubiese gustado hacer aparte de lo que hago hoy día y que si pudiera retroceder en el tiempo hareia lo mismo que hago hoy día: crear vida.
En muchas oportunidades cuando me encuentro dentro de mi laboratorio de fertilidad siento que no podría estar en otro sitio donde esté mas feliz. Es una sensación única de plena paz. En ese lugar puedo meditar, siento vida y encuentro el sentido para muchas de mis interrogantes. Cuando miro mi vida hacia atrás pienso que no existe nada mas que me hubiese gustado hacer aparte de lo que hago hoy día y que si pudiera retroceder en el tiempo hareia lo mismo que hago hoy día: crear vida. Dentro de nuestro laboratorio de embriología tenemos un ambiente ameno con música que varía desde la clásica hasta el rock y pop. He observado como nuestros embriones se comportan de formas distintas ante los diversos geeneros musicales y hasta con el hecho de tener o no música durante su proceso de división dentro de las incubadoras durante las noches. Todos los días coloco música cuando tenemos embriones dentro de nuestras incubadoras y los cambios son bastante significativos. Como es esto posible? Aún no tengo una respuesta científicamente concreta. Es posible que los embriones tengan percepción del ambiente que los rodea? Absolutamente. Esto sí tiene su explicacieon científica con el hecho de que deben existir condiciones adecuadas dentro de las incubadoras donde se encuentran los embriones y dentro del mismo laboratorio de embriología donde habitan por 3 a 6 días. Estas condiciones inciden de forma directa en los procesos de división de los mismos y por ende afectan su calidad.
Dentro de nuestro laboratorio de embriología tenemos un ambiente ameno con música que varía desde la clásica hasta el rock y pop. He observado como nuestros embriones se comportan de formas distintas ante los diversos geeneros musicales y hasta con el hecho de tener o no música durante su proceso de división dentro de las incubadoras durante las noches. Todos los días coloco música cuando tenemos embriones dentro de nuestras incubadoras y los cambios son bastante significativos. Como es esto posible? Aún no tengo una respuesta científicamente concreta. Es posible que los embriones tengan percepción del ambiente que los rodea? Absolutamente. Esto sí tiene su explicacieon científica con el hecho de que deben existir condiciones adecuadas dentro de las incubadoras donde se encuentran los embriones y dentro del mismo laboratorio de embriología donde habitan por 3 a 6 días. Estas condiciones inciden de forma directa en los procesos de división de los mismos y por ende afectan su calidad. Una anécdota graciosa se refiere a pacientes que cuando nos llevan a los bebés para conocerlos nos comentan que reconocen de alguna forma mi voz mientras se encuentran en la sala de espera y me escuchan conversando dentro. No me han conocido en persona aún pero mi voz les suena conocida. Como es esto posible? Pues mi teoría es que me recuerdan de alguna forma.
Una anécdota graciosa se refiere a pacientes que cuando nos llevan a los bebés para conocerlos nos comentan que reconocen de alguna forma mi voz mientras se encuentran en la sala de espera y me escuchan conversando dentro. No me han conocido en persona aún pero mi voz les suena conocida. Como es esto posible? Pues mi teoría es que me recuerdan de alguna forma.![Facebook-y-Twitter[1]](https://fertiaguerrevere.com/wp-content/uploads/2013/12/Facebook-y-Twitter1-e1388000375648.jpg) A través de este artículo la familia de FERTIAGUERREVERE desea extenderle un saludo a toda la comunidad de pacientes que nos acompaña en nuestro trayecto tan maravilloso de brindar vida y esperanzas. Creemos en la medicina basada en evidencias y eso precisamente es lo que hemos venido compartiendo con ustedes en nuestros artículos de la web y publicaciones de nuestro Facebook y Twitter. Nos sentimos muy complacidos por contar con un número de seguidores de Twitter por encima de 14.000 y la aceptación en nuestro Facebook. La idea es transmitir la mayor cantidad posible de información que pueda proporcionar conocimientos relacionados con el maravilloso mundo de la Reproducción Asistida.
A través de este artículo la familia de FERTIAGUERREVERE desea extenderle un saludo a toda la comunidad de pacientes que nos acompaña en nuestro trayecto tan maravilloso de brindar vida y esperanzas. Creemos en la medicina basada en evidencias y eso precisamente es lo que hemos venido compartiendo con ustedes en nuestros artículos de la web y publicaciones de nuestro Facebook y Twitter. Nos sentimos muy complacidos por contar con un número de seguidores de Twitter por encima de 14.000 y la aceptación en nuestro Facebook. La idea es transmitir la mayor cantidad posible de información que pueda proporcionar conocimientos relacionados con el maravilloso mundo de la Reproducción Asistida.

 El cáncer de mama es una patología que se ha convertido en una gran angustia para todas las mujeres. Es difícil pensar que no sea de esta manera para alguna mujer de esta época, y eso, es muy bueno, porque traduce la buena labor que se está llevando a cabo por todas esas maravillosas organizaciones que luchan contra este gran flagelo que cada día le gana más terreno a la vida. El cáncer de mama es una de las primeras causas de mortalidad en nuestro país, la primera es el cáncer de cuello uterino, luego el cáncer de pulmón, cáncer de colon seguido del cáncer de mama.
El cáncer de mama es una patología que se ha convertido en una gran angustia para todas las mujeres. Es difícil pensar que no sea de esta manera para alguna mujer de esta época, y eso, es muy bueno, porque traduce la buena labor que se está llevando a cabo por todas esas maravillosas organizaciones que luchan contra este gran flagelo que cada día le gana más terreno a la vida. El cáncer de mama es una de las primeras causas de mortalidad en nuestro país, la primera es el cáncer de cuello uterino, luego el cáncer de pulmón, cáncer de colon seguido del cáncer de mama.
 No quiero sentirme mas impotente, cuando una mujer o su pareja nos llama y nos dice, después de haber pasado un poco la angustia por esta noticia, “ya llevo tres o cuatro ciclos de quimio, mi cáncer gracias a Dios no es tan fuerte, pero quiero vitrificar mis óvulos, o congelar mis embriones…”, acá , ya es poco, por no decir nada lo que se puede hacer, el mensaje es: no se desesperen colegas médicos, pacientes y familiares, piensen en positivo, las muertes por el cáncer de mama en nuestro país no aumentan porque tenemos un cáncer más agresivo, pasan porque o no diagnosticamos a tiempo, o porque no contamos con los insumos necesarios, esto nos compromete a ayudar mas a esas fundaciones dentro de las cuales hoy día está la nuestra ONCOFERTI, y muchas otras, para prevenir, curar y recordar que la meta es la vida del paciente, y permitirle dar vida después de salir de esta enfermedad.
No quiero sentirme mas impotente, cuando una mujer o su pareja nos llama y nos dice, después de haber pasado un poco la angustia por esta noticia, “ya llevo tres o cuatro ciclos de quimio, mi cáncer gracias a Dios no es tan fuerte, pero quiero vitrificar mis óvulos, o congelar mis embriones…”, acá , ya es poco, por no decir nada lo que se puede hacer, el mensaje es: no se desesperen colegas médicos, pacientes y familiares, piensen en positivo, las muertes por el cáncer de mama en nuestro país no aumentan porque tenemos un cáncer más agresivo, pasan porque o no diagnosticamos a tiempo, o porque no contamos con los insumos necesarios, esto nos compromete a ayudar mas a esas fundaciones dentro de las cuales hoy día está la nuestra ONCOFERTI, y muchas otras, para prevenir, curar y recordar que la meta es la vida del paciente, y permitirle dar vida después de salir de esta enfermedad. Así inicia la gran mayoría de las consultas de Fertilidad, “CULPA”, es la palabra que recomiendo a mis pacientes JAMÁS utilizar. cuando se habla de culpa, se le da un tinte muy cruel e injusto al verdadero propósito de la consulta, yo sugiero cambiar “CULPA por CAUSA’, de esta manera, la pregunta al llegar a la consulta sería, ¿donde esta la causa por la que aún no tenemos hijos”.
Así inicia la gran mayoría de las consultas de Fertilidad, “CULPA”, es la palabra que recomiendo a mis pacientes JAMÁS utilizar. cuando se habla de culpa, se le da un tinte muy cruel e injusto al verdadero propósito de la consulta, yo sugiero cambiar “CULPA por CAUSA’, de esta manera, la pregunta al llegar a la consulta sería, ¿donde esta la causa por la que aún no tenemos hijos”. El propósito de la consulta de fertilidad es lograr traer un niño a casa, esa cosita que va a llenar de luz su hogar, a cambiar completamente el ritmo de sus vidas para bien, si usted, no tiene esa idea clara, debe analizarlo mejor, deben sentir que están emprendiendo una carrera llena de obstáculos que solo se pueden vencer si trabajamos en equipo, porque el premio es maravilloso. Cuando nos sentamos en el consultorio y decimos “nos gustaría seber cuál es la causa por la que aun no hemos logrado tener un bebe”‘ y más aún, si alguno de los dos tiene alguna causa conocida, usted esta abierto a escuchar, dispuesto a someterse a las pruebas que sean necesarias para lograr lo que busca, además, no imagina como le facilita el trabajo a nuestros médicos, quienes muchas veces sentimos que estamos en un ring de boxeo frente a dos enemigos que buscan llevarse la corona de la “No CULPA’
El propósito de la consulta de fertilidad es lograr traer un niño a casa, esa cosita que va a llenar de luz su hogar, a cambiar completamente el ritmo de sus vidas para bien, si usted, no tiene esa idea clara, debe analizarlo mejor, deben sentir que están emprendiendo una carrera llena de obstáculos que solo se pueden vencer si trabajamos en equipo, porque el premio es maravilloso. Cuando nos sentamos en el consultorio y decimos “nos gustaría seber cuál es la causa por la que aun no hemos logrado tener un bebe”‘ y más aún, si alguno de los dos tiene alguna causa conocida, usted esta abierto a escuchar, dispuesto a someterse a las pruebas que sean necesarias para lograr lo que busca, además, no imagina como le facilita el trabajo a nuestros médicos, quienes muchas veces sentimos que estamos en un ring de boxeo frente a dos enemigos que buscan llevarse la corona de la “No CULPA’ Mí recomendación para cada pareja que empren esta maravillosa búsqueda, no acudan a la consulta de fertilidad molestos ni obligados, hagalo cuando de corazón estén dispuestos a buscar la CAUSA, a sentir que van al lado de la persona que aman y la que apoyaran en todo momento, independientemente de cuan escabroso sea el camino, sientan que van a buscar lo mas hermoso de sus vidas, un ser que los unirá cada día mas y sobre todo, que los hará cada día mejores personas. “esos son los pacientes que nos irradian con su optimismo”, y quienes con toda seguridad reciben la bendición del todo poderoso, porque la vida es de Dios, y nosotros solo somos instrumentos en el milagro de la vida.
Mí recomendación para cada pareja que empren esta maravillosa búsqueda, no acudan a la consulta de fertilidad molestos ni obligados, hagalo cuando de corazón estén dispuestos a buscar la CAUSA, a sentir que van al lado de la persona que aman y la que apoyaran en todo momento, independientemente de cuan escabroso sea el camino, sientan que van a buscar lo mas hermoso de sus vidas, un ser que los unirá cada día mas y sobre todo, que los hará cada día mejores personas. “esos son los pacientes que nos irradian con su optimismo”, y quienes con toda seguridad reciben la bendición del todo poderoso, porque la vida es de Dios, y nosotros solo somos instrumentos en el milagro de la vida.